Craniosacral osteopathy
Craniosacral osteopathy By Torsten Liem

History of Craniosacral osteopathy
Osteopathy, developed at the end of the last century by A.T. Still. With its claim to being a holistically oriented healing system, is classified by the use of hands to heal diseases.
All principles of osteopathy are based on the unity of the organism, its self-regulatory and healing forces, the reciprocal influence of the body structure, or tissue, and their function, or physiology, the importance of circulation, as well as putting these insights into practice.
The concept of craniosacral osteopathy was developed at the beginning of the 1930s by William Garner Sutherland. It consists of the application of osteopathic principles on the skull. In addition to the heart rate and the respiratory rhythm, craniosacral osteopathy integrates another rhythmic phenomenon with homeostatic effects called the Primary Respiratory Mechanism. It also refined the skills to release tight body structures with very fine impulses.
Osteopathy
Osteopathy does not primarily deal with special techniques. That is why the founder, A.T. Still, has rarely described any techniques in his various publications. Each osteopath will have the capability of developing his own techniques in his practice, which adapt to the individual needs of the patient.
Osteopathy is a specific view point, which enables certain therapeutic procedures to release restricted motion, to enable unrestricted circulation, nerve and energy supply and to release resources which allow healing in the best possible way. Therefore, the art of practicing Osteopathy, which means the consciously done palpation, is based on a philosophic and scientific foundation.

Through palpatory perception of normality or of homeostatic forces, the Craniosacral osteopathy tries to get close to the wholeness of the patient. Above all, the first and most important foundation for the osteopath is the sensory experience of normality, meaning the health in the tissue. That is not a mechanical or technocratical palpation, but a deep, subjective experience, which, according to Sutherland can be experienced most clearly in a state of stillness.
I especially want to recommend the following publications:
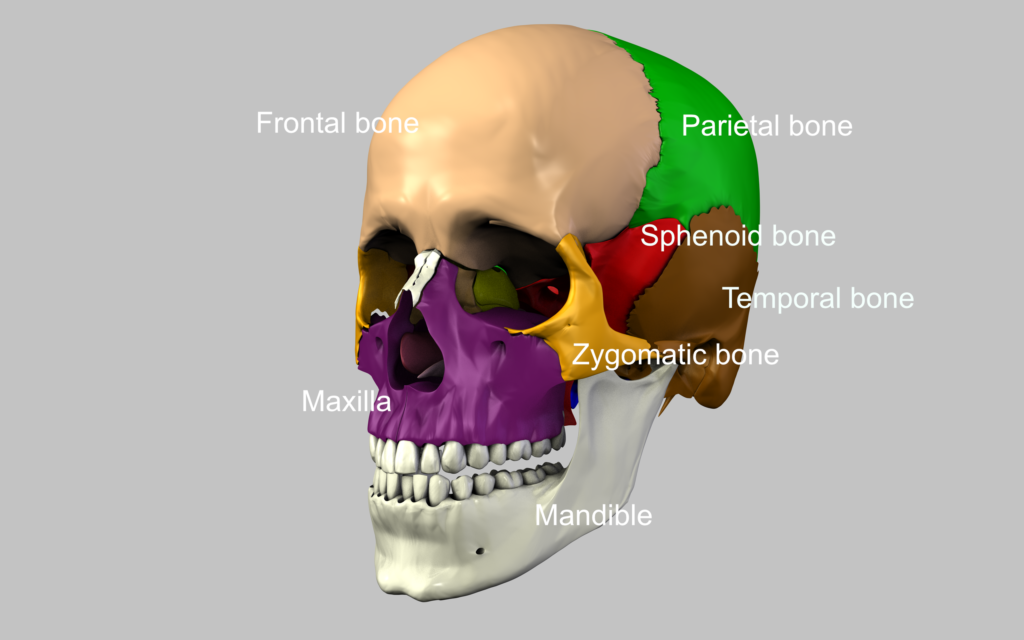
The following part shows the bones of the skull and important anatomical structures.
Ossification:
Capital bone:
Lower part of the occipital bone including the supra-occiput develoaps from cartilaginous tissue.
The inter-parietal occiput develops from membranous tissue.
Temporal bone:
Petrous portion is the evolution from cartilage.
The squamous portion and the tympanic portion develop from membran.
The petrous portion is the part of the skull which ossifies first. In the 22nd foetal week the ossification of the auditory system is already completed. At birth the squamous portion and the tympanic portion are already partly connected, forming the tympano-squamous fissure, which can be a possible location for intraosseous dysfunctions.
The squamous portion, the petrous portion and the styloid process melt together during the first year.
The mastoid process doesn’t develop until after the second year and can not be palpated on a newborn.
Ethmoid bone:
The ethmoid bone and the vomer develop from cartilage.
Sphenoid bone:
Both pterygoid processes and the upper part of the greater wings develop from membranous tissue.
Frontal bone:
The frontal bone develops from membranous tissue. Only the nasal spine develops from cartilaginous tissue.
In 85 to 90% of the cases, the metopic suture ossifies by the 7th year.
Parietal bone:
The parietal bone ossifies from membrane. There is one ossification centre located in each parietal eminence.
Maxilla and pre-maxilla are formed from membrane between the 7th and 8th foetal week.
The other bones also develop from membranous tissue.
Points of Orientation on the skull
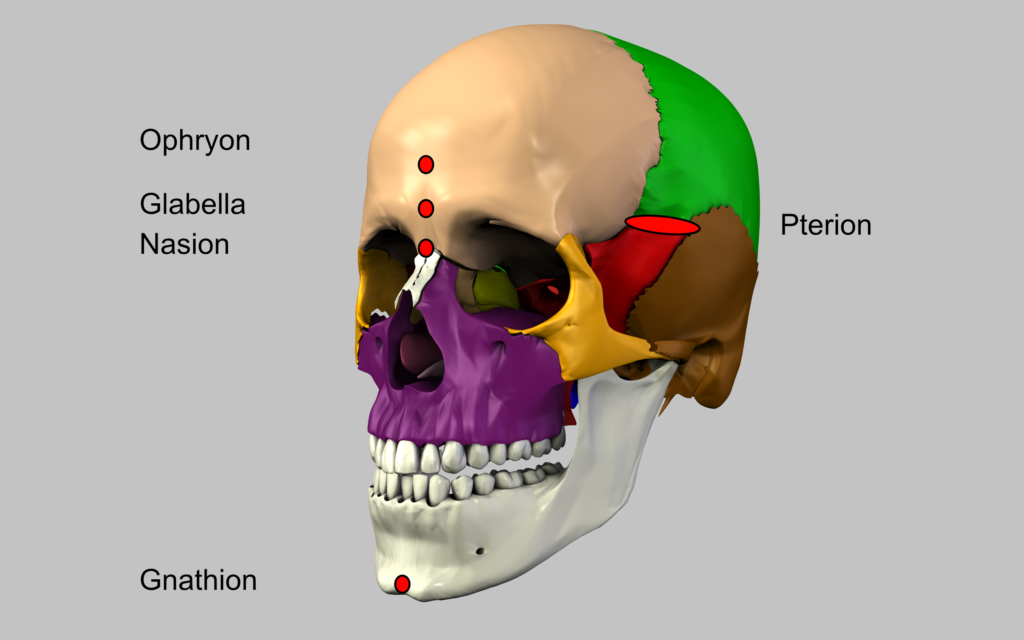
1. Gnathion is a median point on the tip of the chin of the lower jaw
11. Basion is a median point at the anterior rim of the foramen magnum
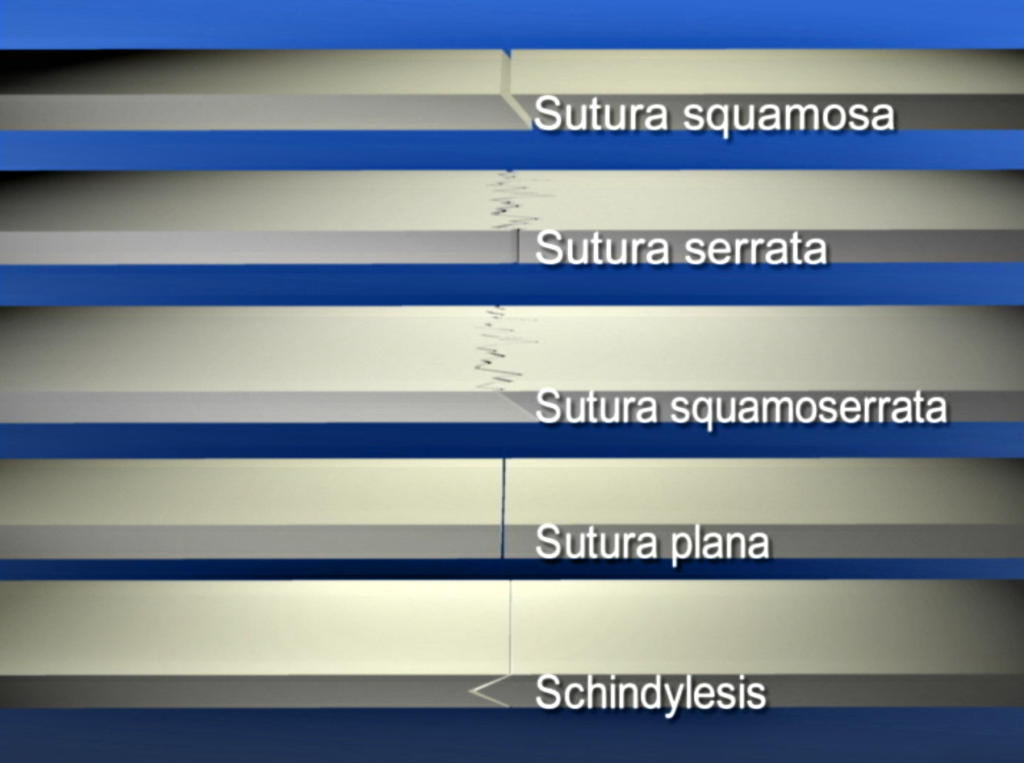
Sutures
Coronal & Spheno Suture
- At the coronal suture, the frontal bone overlaps the parietal bone in the medial part. Pass the time the parietal bone overlaps the frontal bone in the lateral part.
- At the spheno-frontal suture the greater wings of the sphenoid overlap the frontal bone
- At the spheno-squamous suture the temporal bone overlaps the greater wing of the sphenoid in its portrayed vertical part. One can not see how the greater wing of the sphenoid covers the temporal bone in its horizontal part.
Spheno & Parieto Suture
- At the spheno-parietal suture the parietal bone is covered by the sphenoid bone.
- At the parieto-squamous suture the temporal bone generally covers the parietal bone. In the anterior part it is possible, that the borders switch and that the parietal bone overlaps the temporal bone.
- At the parieto-mastoid suture the temporal bone covers the parietal bone. It is also possible, that the parietal bone is bevelled medially at the anterior end and therefore overlaps the temporal bone.
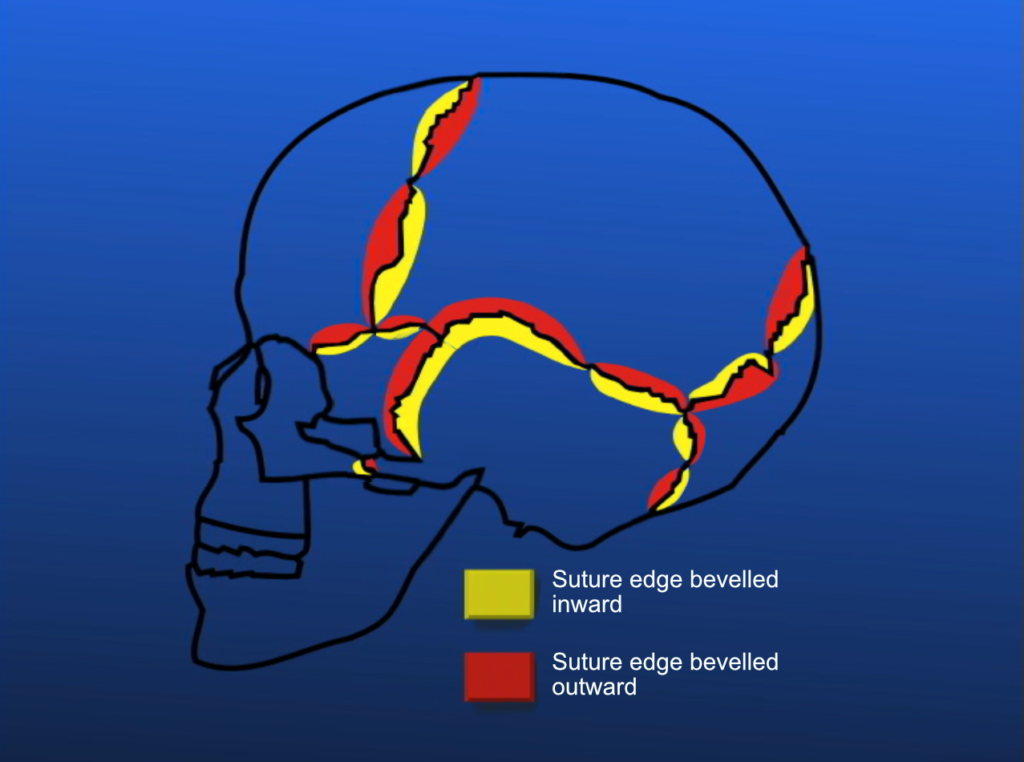
- At the lambdoid suture the occipital bone overlaps the medial part of the parietal bone. While the parietal bone overlaps the occipital bone in the lateral part.
- occipito-mastoid suture the temporal bone overlaps the occipital bone in the cranial part.
- In the caudad portion the occipital bone overlaps the temporal bone. This however does not occur regularly. The change of the overlapping is called condylo-squamo-mastoid pivot point.
- At the temporo-zygomatic suture the temporal bone is usually overlapped by the zygomatic bone.
- At Pterion the sutures overlap. So at the bottom is the frontal bone, followed by the parietal bone and the sphenoid bone. At the surface is the temporal bone. To help you remember you can use the alphabetical order of the participating bones: F,P,S,T. Pterion is a relatively fixated zone
- At Asterion the occipital bone is at the bottom, followed by the parietal bone and the temporal bone is on top. In contrast to Pterion, Asterion is a relatively mobile zone.
Palpation of the sutures
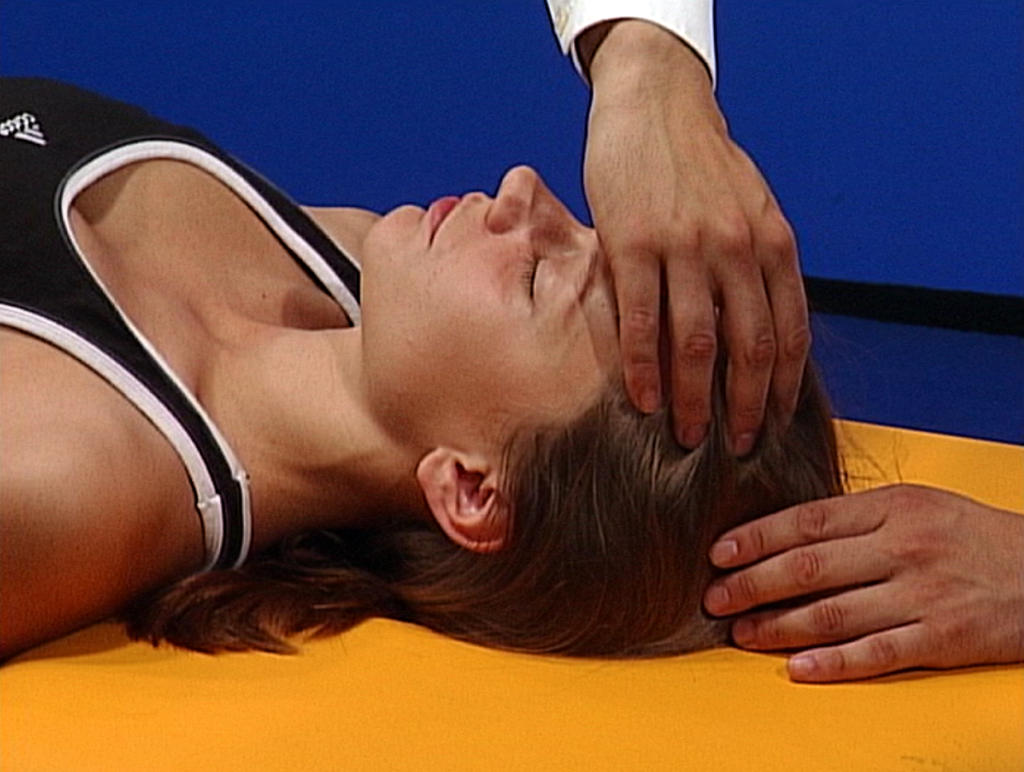
- coronal suture: Palpate with both fingers from the forehead posterior until you perceive a fine furrow (groove, channel) or less often a protrusion. After that, you follow this from medial to lateral until about 2 finger’s width posterior of the lateral edge of the eye.
- At the end of the sagittal suture you palpate an indentation at the back of the skull: Lamda.
- Now palpate Asterion, the joining point of the occipital bone, the parietal bone and the temporal bone, which is located about 2 finger’s width behind and 1 to 2 finger’s width above the ear’s hole (concha). Asterion is a fairly mobile zone, compared to Pterion.
- In the middle of the coronal suture is a little indentation, Bregma. Bregma is about the same distance from the hairline as the hairline is from the eyebrow.
- About to finger’s width posterior to Bregma, on the sagittal suture lies vertex, the highest point of the skull.
- The connecting line between Asterion and Lambda is the lamdoid suture.
- Palpate the occipito-mastoid suture caudally from Asterion along the posterior ridge of the mastoid portion.
Contents

5 videos to download or DVD’s or streaming with integrated menu control
total 323min
Video 1:
- Basics and Palpation
- Anatomy and Ossification of the skull bones
- The Anatomy of the dura mater
- Palpation of the sutures
- Primary Respiration
- Biomechanics and Biodynamic
- Vault hold
Video 2:
- Diagnosis- and Treatment Principles / Techniques
- Diagnosis- and Treatment Principles
- Fluctuation techniques
- Venous sinus techniques
- Dura techniques
Video 3:
- Neurocranium
- SBS: Anatomy, Diagnosis and Treatment
- Sutures of the frontal bone
- The Sutures of the temporal bone
- Sutures of the parietal bone
- Intraosseous treatment
Video 4:
- Viscerocranium
- Sutures of the frontal bone
- The Sutures of the Maxilla
- Sutures of the Palatine bone
- The Sutures of the Zygomatic bone
- Sutures of the Ethmoid bone
- The Sutures of the Vomer
- Sutures of the Nasal bone and lacrimal bone
- General Treatment of the Viscerocranium
Video 5:
- Viscerocranium Part 2 and Treatment of the Midline
- The Sutures of the frontal bone •Sutures of the Maxilla
- Sutures of the Palatine bone
- The Sutures of the Zygomatic bone
- Sutures of the Ethmoid bone
- The Sutures of the Vomer
- Sutures of the Nasal bone and lacrimal bone
- General Treatment of the Viscerocranium
- Pterygopalatine ganglion
- Treatment of the Midline
- Treatment of geometric lines